Myocarditis Higher After Receiving a COVID Vaccine, New Data Show

This was the key figure in a Nature Medicine paper published on Dec. 14, 2021. It showed clearly that myocarditis after vaccination (in this case, Moderna dose two) was higher than myocarditis after SARS-CoV-2 infection for people <40.
But the story does not end there….
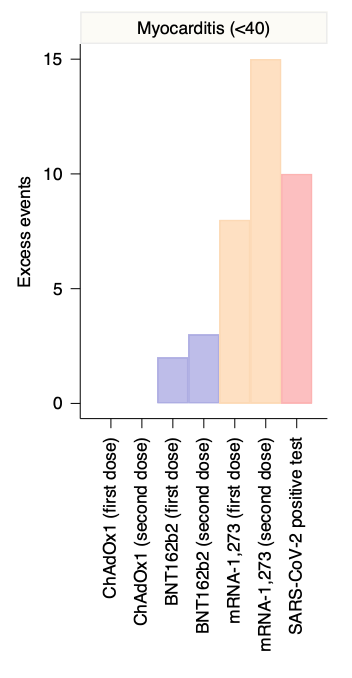
There were a few remaining issues. While the denominator for vaccines is known with precision, the true number of infections is unknown. Many people don’t seek testing or medical care. So the red bar above will be shorter if you used a sero-prevalence (a.k.a the correct) denominator. The authors needed to fix this.
The other problem is that this analysis lumps together men & women, while men have the greatest risk. Well, the authors are back with a new pre-print to fix this point, and here is what they find.
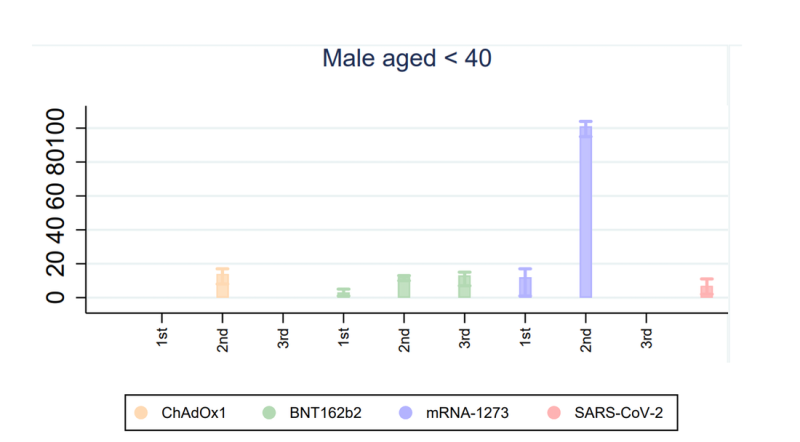
- It is now clear for men <40, dose two and dose three of Pfizer have more myocarditis than SARS-CoV-2 infection, and this is true for dose one and dose two of Moderna.
- Pfizer boosters (dose three) have more myocarditis for men <40 than infection.
- Myocarditis post infection is more common as you get older, in contrast with myocarditis post vaccination, which is more common as you are younger (reverse gradients).
But the truth is STILL WORSE than these data.
- If the authors fixed the denominator for viral infection (i.e. used sero-prevalance), it would look even worse.
- If the authors separate men 16-24 from 12-15 and 25-40, it would likely look worst in 16-24 age group.
But regardless, these findings already clearly dispel the true misinformation online: Yes, sorry to break it to you, vaccines can have risks of myocarditis exceeding risks of myocarditis from infection. Please stop saying otherwise.
And here is why it matters:
- There is marked uncertainty as to whether dose three actually lowers severe outcomes and hospitalizations in young men. The FDA is making a huge regulatory gamble with boosters, and they are cheered on by many who are not adept at data analysis.
- Boosting 16-40 year old men might not be in their best interest (it might be net detrimental). We simply do not know with confidence. If it is revealed that it is not in their best interest, this administration will have dropped a nuclear bomb on vaccine confidence for 20 years. God help us all.
- We could have spaced out dose two in young men, or considered omitting it entirely, as some colleagues and I have been saying since June, in an effort to capture most of the gains and eliminate most of the harms of vaccination. This can still be done for Pfizer.
- The US FDA must halt use of Moderna in Men <40, as other nations have. Just like they dragged their feet with J&J and VITT, they drag their feet here, and people needlessly suffer due to their inaction.
These new data are of immediate and vital interest. Vaccination is important, but maximizing benefit and minimizing harms is the key. I do not see that the agencies meant to do this are pursuing it in the US.
Perhaps that is why Marion Gruber and Phil Krause, the Director and Deputy Director of vaccine products at FDA, resigned: they wanted no part of this.
Republished from the author’s Substack.